- Research
- Open access
- Published:
Prevalence of depression and anxiety among working women in Saudi Arabia: psychosocial and perinatal correlates
BMC Women's Health volume 25, Article number: 228 (2025)
Abstract
Background
Women comprise a sizeable portion of the workforce in various industries. They might face many challenges that affect their mental well-being. Hence, a study that addresses working women’s psychosocial and perinatal aspects mandates the necessity to fill the void and deficiencies related to clinical research.
Objectives
To explore the prevalence of depression and anxiety among working women in Saudi Arabia and its psychosocial and perinatal correlations.
Methods
This cross-sectional study involved 580 working women from Riyadh, Saudi Arabia, who participated via convenience sampling. An online-based questionnaire was used to collect data, including sociodemographic, occupational, medical, and perinatal data. The Patient Health Questionnaire (PHQ-9) and Generalized Anxiety Disorder 7 (GAD-7) were used to assess depression and anxiety.
Results
More than half (56.4%) had a pregnancy history, half of them took maternity leave (49%), and most needed additional leave (65.2%). Half of the participants had mild to moderate levels of depression and anxiety, 50.2% and 49%, respectively. A positive correlation was found between depression and anxiety (p-value = < 0.001). Participants who drank alcohol or had a lower mean score of total pregnancies had a significantly higher prevalence of moderately severe to severe depression (p = < 0.05). And smokers had a significantly higher rate of severe anxiety (p = < 0.01). Participants previously diagnosed with a psychiatric disorder displayed a higher risk of severe depression and anxiety (p < 0.001).
Conclusion
The findings of this study highlight the significant prevalence of mild to moderate level of depression and anxiety among working women in Saudi Arabia and their strong association with various psychosocial and perinatal factors. These results underline the urgent need for comprehensive mental health support and interventions tailored to the unique challenges faced by working women in the region.
Introduction
Mental health among working women in Saudi Arabia has risen over the recent years, sharing global concerns but with its own regional characteristics. Despite facing socio-cultural and occupational challenges, there has been a significant increase in the employment of Saudi women. In 2021, the General Authority for Statistics in Saudi Arabia (GASTAT) reported the total number of workers to be 13,483,813 persons, where women’s participation in the labor market increased to 36% [1]. This reflects a significant growth in economic participation even as half of the Saudi population grapples with mental illness driven by these challenges [2], while the Saudi Arabia Mental Health Surveillance System (2021) highlights significant trends in anxiety and depression among women during the COVID-19 pandemic [3]. Further insights emphasize the ongoing national efforts to screen and address these mental health issues, indicating a growing awareness and institutional acknowledgment of the problem [4], with a correlation between workplace demands and increased anxiety and depression among pregnant working women in Saudi Arabia [5].
The Kingdom of Saudi Arabia has made dramatic changes and implemented policies and rules to empower women in the workplace and to ensure their rights, safety, equality, and well-being. Despite these tremendous efforts to protect women and their well-being, the mental health of working women remains an active area that demands to be acknowledged, understood and improved. In Saudi Arabia, data on the mental health of working women is virtually non-existent.
Regionally, psychosocial challenges faced by Arab working women shed light on the additional burdens of societal expectations and familial responsibilities, which compound workplace stressors and impact mental health [6]. These findings align with the psychological distress faced by healthcare workers, including a high prevalence of depression and anxiety in other Arab countries like Egypt as well [7]. Another study recruited a sample of 101 Jordanian working women and reported that more than half of these women complained of moderate to severe depressive symptoms. Their study concluded that the causes of women’s depressive symptoms were embedded in their familial and social environment rather than their jobs per se [8].
Mental health issues are a growing public health concern. They are a major source of disability and dependency, affecting individuals’ well-being and quality of life. The World Health Organization estimates that 25% of the global population suffers from mental illnesses in both developed and developing countries [9, 10]. Recognizing the urgency, mental health has been incorporated into the UN Sustainable Development Goals (SDGs) and identified as a priority for global development over the next 15 years [11].
Work itself may not be considered the sole cause of mental health problems. Still, unfavorable working conditions can undoubtedly decompensate a vulnerable mental health status with other risk factors and stressors. These influential factors and stressors must be identified to protect, safeguard, and improve women’s mental health at work. Research has shown that participants exposed to high psychological job demands had a two-fold risk of major depressive disorder or generalized anxiety disorder compared to those with low job demands [12].
Previous literature reported that women face many environmental, domestic, and working challenges that affect their mental well-being and are more vulnerable than men to mental health problems [13]. Depression and anxiety, particularly, have not only been more prevalent in women than in men but are also more disabling [14,15,16]. Furthermore, low-income working mothers in urban areas of India have been found to struggle significantly with mental health, often exacerbated by factors such as domestic violence and insufficient support [17]. A Spanish manifested poor mental health, which was much more prevalent in women than men. This prevalence amongst women was even higher as age increased among widowed, separated/divorced, and self-employed women [18]. In Korea, 767 employed Korean women were studied. Among those participants, 286 participants were depressed [19]. In Ethiopia, working women had a 2.74-fold higher prevalence of mental distress than men [20]. International studies on the mental health of working women are inconclusive, and this field mandates further research to fill its void.
According to the Centers for Disease Control and Prevention, about 1 in 10 women in the United States reported symptoms that suggest they experienced an episode of major depression in the last year, and about 1 in 8 women with a recent live birth experience symptom of postpartum depression [21]. Across diverse countries and social contexts, mental health problems, particularly depression and anxiety, affect women more than men [3, 4, 22, 23]. Many epidemiological studies confirmed high comorbidity between anxiety and depression, thus suggesting a close connection between them [24, 25]. The two illnesses have frequently been the focus of research for numerous organizations in various local and international contexts. This study aims to explore the prevalence of depression and anxiety among working women in Saudi Arabia and its psychosocial and perinatal determinants.
Subjects and methods
Design and setting
This cross-sectional study was conducted in Saudi Arabia from May to August 2022, focusing exclusively on the working female population in Riyadh, both in the private and public sectors.
Participants and recruitment
The study included employed females residing in Riyadh, Saudi Arabia. The exclusion criteria were unemployed or retired females and those not living in Saudi Arabia. Non-Saudi women living and working in Riyadh were also included. The sample size was calculated using Raosoft software and estimated at the 95-confidence level with an estimated 50% response distribution and a margin of error of ± 5%. The recommended sample size is 384.
Ethical considerations
The study was conducted upon the approval of the Institutional Review Board (IRB) of Princess Nourah Bint Abdulrahman University, Saudi Arabia (IRB log number: 21–0494). Informed consent was obtained from all participants after a brief explanation of the study’s objectives, and they were informed that they had the full right to withdraw from the study without any obligation.
Data collection instruments and procedures
The sampling was based on a convenient nonprobability sampling technique. An online questionnaire was sent to working women through their respective institutions via an official email or phone number.
The questionnaire was segmented into five sub-sections: (1) Demographic data that includes age, gender, nationality, region of living, marital status, number of children, educational level, medical or psychiatric condition, smoking status, substance use, and drinking alcohol. (2) Occupational data includes occupation, type of work sector, years of work experience, monthly income, and number of working hours per week. (3) Medical and perinatal data includes the number of previous pregnancies, pregnancy complications, delivery complications, postpartum depression, time taken until returning to work, and concealing pregnancy during work. (4) Study Instruments: The Patient Health Questionnaire (PHQ-9) and the Generalized Anxiety Disorder 7 (GAD-7) were used to assess depression and anxiety, respectively, employing a 3-Likert scale for responses. PHQ-9 and GAD-7 were translated into Arabic by certified translators, and their validity and reliability for the Arabic-speaking population have been previously established with Cronbach’s alpha (α = 0.89 and 0.95, respectively) [26]. The PHQ-9 consists of nine items, and scores are typically categorized as follows: mild depression (score of 5–9), moderate depression (score 10–14), moderately severe depression (score 15–19), or severe depression (score 20–27). The GAD-7 consists of seven items, and scores are typically categorized as follows: mild anxiety (score of 5–9), moderate anxiety (score 10–14), or severe anxiety (score 15–21) [26].
Data management and analysis
Data were analyzed using SPSS version 26; qualitative data were expressed as numbers and percentages using the Chi-squared test (χ2) to examine the relationships between variables, while quantitative data were expressed as mean and standard deviation (Mean ± SD), with non-parametric variables tested using the Kruskal-Wallis test. Correlation analysis was performed using Spearman’s test, considering a p-value of less than 0.05 as statistically significant. The sample size, calculated using Raosoft software, was determined based on a 95% confidence level, an estimated 50% response distribution, and a margin of error of ± 5%, recommending a total of 384 participants.
Results
Table 1 shows that the mean age of the studied participants was 32.17 ± 7.57 years, and the mean number of children was 1.61 ± 1.87. The majority had a Saudi nationality (98.6%) and a bachelor’s degree in education (67.4%) and were married (66.2%). Third of the participants had a healthcare job (34.7%), while one-quarter had an office or administrative job (25.7%). Most study subjects worked in the public sector (66.6%) with 7.08 ± 6.48 years of work experience. Almost a third had a monthly income of 11,000–20,000 Saudi Riyal (32.6%), and the majority had a full-time 40–45 h of work (62.6%). Moreover, 15.3% of participants had chronic diseases, and 14.8% of them had psychiatric disorders, with anxiety (70.9%) being the most common disorder. Only 6.2% were smokers, 0.2% used recreational drugs, and 2.1% drank alcohol. More than half (56.4%) had a pregnancy history, 13.6% were currently pregnant, and 38.1% were in the 2nd trimester. The mean previous pregnancies were 2.64 ± 2.07 pregnancies. Half of the participants took maternity leave (49%), and out of them, 65.2% needed additional leave.
The mean scores of PHQ-9 and GAD-7 were 8.33 ± 5.67 and 8.74 ± 6.14, respectively. Figure 1 illustrates that among studied women, the prevalence of minimal, mild to moderate, and moderately severe to severe depression was 29.5%, 50.2%, and 20.3%, respectively. Furthermore, Fig. 2 depicts that the prevalence of minimal, mild to moderate and severe anxiety was 35.5%, 49%, and 15.5%, respectively.

Percentage distribution of depression status based on the PHQ-9 scores classification

Percentage distribution of anxiety status based on the GAD-7 scores classification
Tables 1 and 2 demonstrate the relationship between depression and anxiety regarding various variables. There was no significant relationship with sociodemographic or occupational variables (p-value = > 0.05). Participants who were diagnosed previously with a psychiatric disorder had a significantly higher percentage of severe depression and anxiety (p = < 0.001). The prevalence of moderately severe to severe depression was significantly higher among those drinking alcohol or having a lower mean score of total pregnancies (p = < 0.05). While severe anxiety was significantly higher among smokers (p = < 0.01).
Figure 3 illustrates a significant positive correlation between the PHQ9 and the GAD-7 scores (r = 0.73, p-value = < 0.001).
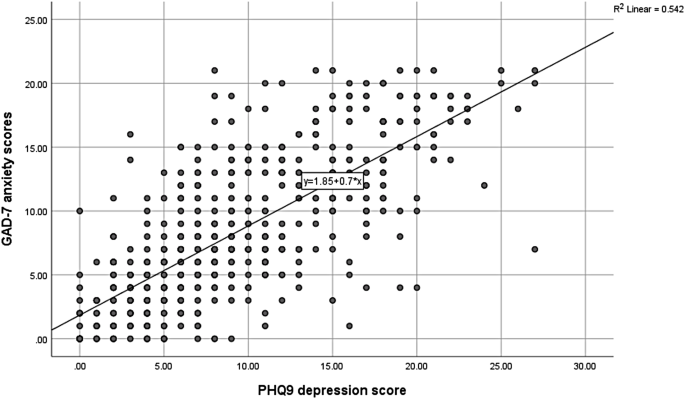
Spearman’s correlation analysis between PHQ9 and GAD-7 scores. N.B.: (r = 0.73, p-value = < 0.001)
Discussion
To our knowledge, this current study is the first to assess depression and anxiety among working women in Saudi Arabia and its psychosocial and perinatal determinants. The prevalence of mild to moderate and moderately severe to severe depression was 50.2% and 20.3%, respectively. The prevalence of mild to moderate and severe anxiety was 49% and 15.5%, respectively. These results are similar to studies in Arab regions like Egypt and Jordan, which reported higher levels of depression and anxiety among working women [8, 27]. An explanation for the congruency of these findings with our results could be attributed to cultural similarities between the study subjects. Many understandable reasons could explain the vulnerable state of this group of women. Gender discrimination, pressure of multiple roles by women, and gender-based violence are all examples of these reasons. The greater housework and caregiving demand required from women compared to men, given their role as the primary caregiver at home in many cultures, can significantly jeopardize their mental health status. Work-related demands associated with full-time jobs, responsibilities at home, including housework, childcare, and social obligations to the family, and possible financial hardship could be sources of stress for this group of women. Women working for long hours could become subject to stressors as they work to meet their job obligations at the expense, sometimes, of their personal needs, children, and families.
In Spain, the prevalence of poor mental health was higher in working women than in men and was more related to socioeconomic rather than work-related variables [18]. In Germany, working women, especially those working in manual occupations, were found to be at a greater risk of poor mental health than men [28]. Furthermore, nightwork and overtime work were significantly correlated with anxiety [6]. As the majority of women in our study were in the healthcare sector, a gender gap of psychological disturbances with a higher prevalence of depression, anxiety, and stress among female healthcare workers than men were similarly documented [7, 29].
On the other hand, many research studies confirmed low levels of anxiety and depression with higher life satisfaction among employed women compared to housewife women [30,31,32,33,34]. In the Eastern province of Saudi Arabia, unemployed women were more likely to have depression than employed women. But employed women had a lower anxiety-trait score than unemployed women [5]. These findings can be explained by the assumption that employed women are usually more educated, financially independent, have more opportunities for making friends, socialize and enjoy leisure time, and have a better sense of how to lead a healthy lifestyle [30,31,32,33,34]. Possible reasons for these disparities include variations in access to mental health services, cultural factors, and socioeconomic differences. However, our study didn’t include a comparison group of unemployed women or housewives.
The present study revealed that the prevalence of moderately severe to severe depression was significantly higher among participants who had lower mean scores of total pregnancies. This result agrees with Holton et al., where mothers reported significantly better subjective well-being and greater life satisfaction than childless women [35]. Another study also found that women with children were less likely to be depressed than women without children [36]. This could be due to the functional impairment caused by the severe depression, which results in avoiding getting pregnant or any activity that might cause any additional burden that could be intolerable. Previous research has found that the severity of anxiety and depression may be one of the causes of human reproductive problems and that emotional disorders affect the secretion of sex cycle hormones and endometrial growth [37].
A positive correlation was found between depression and anxiety in this study, which is explained by the high comorbidity between them [24, 25]. Moreover, participants who were diagnosed previously with a psychiatric disorder had a significantly higher percentage of severe depression and anxiety in our analysis. A possible interpretation of this finding is having a previous history of medical problems might affect the subjects’ perception of their health as weak and feeling more vulnerable to contracting a new disease [38]. A strong association was evident in prior studies documenting a significantly higher prevalence of antenatal depression among those who reported depression diagnoses, needed medical consultations, and were treated for depression [39, 40].
Another finding in our study is the high percentage of severe anxiety among smoking participants. Smoking was associated with a higher degree of depression, anxiety, and stress [6, 41]. This finding is in concordance with what has been reported in another Saudi Arabian study [3, 4, 42, 43]. Recent research suggested that depression appears to be associated with smoking dependence and mediated by neuroticism [44]. The association between smoking and depression was examined in 60,814 study subjects, and it was reported that the strongest association was with comorbid anxiety depression, followed by anxiety, and only marginal depression [45].
Participants in our study drinking alcohol had a higher percentage of moderately severe to severe depression. Depression was the predictor variable of problematic alcohol consumption for women aged 18–34 years, and women aged 35–64 years used alcohol as the predominant coping style [46]. Employed females tended to drink more and exhibit higher ratios of problematic drinking, and the psychological attributes related to their drinking related to a state of anxiety and impulsiveness [47].
Half of the participants in the current study took maternity leave (49%), and most needed additional leave after it ended (65.2%). Taking leave from work provides time for mothers to rest, recover from pregnancy and childbirth, and attend to their child’s health and needs. The need to take additional leaves could indicate that the length of the maternity leave is perhaps insufficient. Although the length of maternity leave was not investigated in the scope of the study, a positive association was shown between the size of maternity leave and the mother’s mental health [48]. Women who took a short leave (6 weeks or less) and were high on marital concerns had the highest depression scores [49]. Full-time working women were interviewed at four months postpartum and showed elevated anxiety compared to their counterparts [49]. Short maternity leave can be conceptualized as a risk factor that, when combined with other factors, places women at greater risk for depression [49, 50]. The new policy in Switzerland extends maternity leave for many women to 14 weeks [48]. A more generous maternity leave during the birth of a first child was associated with reduced depressive symptoms [51]. Findings suggest employed women experience problems in well-being at approximately seven months postpartum and that with more than 15 weeks of leave, time off work positively affected maternal mental health [52].
This study has several limitations. The first is the study’s cross-sectional nature. Second, convenience sampling from one city (Riyadh) limits the generalizability of the results. Third, using an online questionnaire might have led to over and underestimation of certain groups (for example, those without internet access). The study did not include a comparison group or differentiate between types of employment, such as hard or simple work, nor did it assess the adequacy of salaries or specific employment contracts with insurance due to the initial study design focusing on broader employment and mental health outcomes. Additionally, while this study did not specifically categorize participants based on psychological or chronic physical disorders, acknowledging these factors as potential covariates in mental health outcomes is crucial for future research. Lastly, all the study data were self-reported, which may have introduced bias.
Despite these limitations, this study has important practical implications for employed women. Implanting flexible or remote working hours can be beneficial in addition to providing generous maternity leave. It is also important to increase workplace awareness about mental health and provide some resources or wellness programs with access to psychological services.
For future studies, it is recommended that a larger sample size of women with various characteristics recruited from different settings be studied. In addition, predisposing social factors like family and work need to be investigated further to determine whether they affect women’s mental health status in the workplace. Future research studies need to be conducted to comprehend the impact of mental distress on work productivity and to elucidate how gender differences may influence reproductive and other health outcomes related to mental distress. Other variables like employment types and employment contracts need to be considered in future studies to understand better how specific employment conditions affect mental health. Also, future studies should include other regions in Saudi Arabia and a comparison group of unemployed women.
Conclusion
In conclusion, this study showed that half of the employed women in Saudi Arabia had mild to moderate levels of depression and anxiety. It’s essential to intervene to prevent functional impairment as a result of severe depression or anxiety. This study reveals that while sociodemographic and occupational factors did not directly correlate with mental health outcomes among employed women in Saudi Arabia, behaviors such as smoking and alcohol use were significantly associated with higher levels of depression and anxiety. Additionally, women with a history of psychiatric disorders exhibited markedly greater incidences of severe depression and anxiety.
Since employed women represent a substantial and expanding segment of the population, it is pivotal to comprehend how employment impacts their mental health and the myriad of variables affecting women’s psychological well-being in the workplace. Further qualitative research is needed to determine the appropriate methods to achieve higher awareness levels and improve well-being. This study highlights the urgent need for enhanced support systems and awareness programs within employment settings to identify and address mental health issues, including unhealthy behaviors like smoking or alcohol use. Enhancing awareness of depression and anxiety among employed women is crucial to improving women’s comprehension and understanding of these disorders and their ability to recognize and seek assistance. Facilitating life-work balance can be integrated at work by launching on-site childcare and wellness programs such as yoga and mindfulness. Importantly, this research contributes to the prompt mental well-being of working women in Saudi Arabia to achieve workplace policies like flexible work arrangements and maternity leave to support women’s mental health better.
Data availability
No datasets were generated or analysed during the current study.
References
GASTAT Issues Saudi Women’s. Report 2022| General Authority for Statistics [Internet]. [cited 2024 Aug 9]. Available from: https://www.stats.gov.sa/en/news/472
Almutairi AF. Mental illness in Saudi Arabia: an overview. Psychol Res Behav Manag. 2015;47–9.
BinDhim NF, Althumiri NA, Basyouni MH, Alageel AA, Alghnam S, Al-Qunaibet AM et al. Saudi Arabia Mental Health Surveillance System (MHSS): mental health trends amid COVID-19 and comparison with pre-COVID-19 trends. Eur J Psychotraumatol [Internet]. 2021;12(1):1875642. Available from: https://doiorg.publicaciones.saludcastillayleon.es/10.1080/20008198.2021.1875642
Alhabeeb AA, Al-Duraihem RA, Alasmary S, Alkhamaali Z, Althumiri NA, BinDhim NF. National screening for anxiety and depression in Saudi Arabia 2022. Front Public Health. 2023;11:1213851.
Alqahtani AH, Al Khedair K, Al-Jeheiman R, Al-Turki HA, Al Qahtani NH. Anxiety and depression during pregnancy in women attending clinics in a university hospital in Eastern Province of Saudi Arabia: prevalence and associated factors. Int J Womens Health. 2018;101–8.
Abbas MAF, Zaid LZA, Hussaein M, Bakheet KH, AlHamdan. NA. Anxiety and depression among nursing staff at King Fahad medical City, Kingdom of Saudi Arabia. J Am Sci. 2012;8(10):788–94.
Arafa A, Mohammed Z, Mahmoud O, Elshazley M, Ewis A. Depressed, anxious, and stressed: what have healthcare workers on the frontlines in Egypt and Saudi Arabia experienced during the COVID-19 pandemic? J Affect Disord. 2021;278:365–71.
Al-Modallal H, Abuidhail J, Sowan A, Al‐Rawashdeh A. Determinants of depressive symptoms in Jordanian working women. J Psychiatr Ment Health Nurs. 2010;17(7):569–76.
Mental Health Gap Action Programme. (mhGAP) [Internet]. [cited 2024 Aug 9]. Available from: https://www.who.int/teams/mental-health-and-substance-use/treatment-care/mental-health-gap-action-programme
World Health Organization. Mental Health Atlas 2011. World Health Organization [Internet]. 2011 [cited 2024 Aug 9];1–81. Available from: http://www.who.int/mental_health/publications/mental_health_atlas_2011/en/
Votruba N, Thornicroft G, Group FS. Sustainable development goals and mental health: learnings from the contribution of the fundamentalsdg global initiative. Global Mental Health. 2016;3:e26.
Melchior M, Caspi A, Milne BJ, Danese A, Poulton R, Moffitt TE. Work stress precipitates depression and anxiety in young, working women and men. Psychol Med. 2007;37(8):1119–29.
Malhotra S, Shah R. Women and mental health in India: an overview. Indian J Psychiatry. 2015;57(Suppl 2):S205–11.
Kessler RC. Epidemiology of women and depression. J Affect Disord. 2003;74(1):5–13.
McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res. 2011;45(8):1027–35.
Abate KH. Gender disparity in prevalence of depression among patient population: a systematic review. Ethiop J Health Sci. 2013;23(3):283–8.
Travasso SM, Rajaraman D, Heymann SJ. A qualitative study of factors affecting mental health amongst low-income working mothers in Bangalore, India. BMC Womens Health. 2014;14:1–11.
Arias-de la Torre J, Artazcoz L, Molina AJ, Fernández-Villa T, Martín V. Inequalities in mental health in the working population of Spain: a National health Survey-based study. Gac Sanit. 2016;30:339–44.
Nam KA, Kim S, Lee H, Kim HL. Employed women with depression in Korea. J Psychiatr Ment Health Nurs. 2011;18(2):139–45.
Gelaye B, Lemma S, Deyassa N, Bahretibeb Y, Tesfaye M, Berhane Y, et al. Prevalence and correlates of mental distress among working adults in Ethiopia. Clin Pract Epidemiol Ment Health. 2012;8:126.
Symptoms of Depression Among Women.| Reproductive Health| CDC [Internet]. [cited 2024 Sep 15]. Available from: https://www.cdc.gov/reproductive-health/depression/index.html
Gelaye B, Arnold D, Williams MA, Goshu M, Berhane Y. Depressive Symptoms Among Female College Students Experiencing Gender-Based Violence in Awassa, Ethiopia. J Interpers Violence [Internet]. 2008;24(3):464–81. Available from: https://doiorg.publicaciones.saludcastillayleon.es/10.1177/0886260508317173
Richardson LK, Amstadter AB, Kilpatrick DG, Gaboury MT, Tran TL, Trung LT et al. Estimating Mental Distress in Vietnam: the Use of the SRQ-20. International Journal of Social Psychiatry [Internet]. 2010;56(2):133–42. Available from: https://doiorg.publicaciones.saludcastillayleon.es/10.1177/0020764008099554
Jacobson NC, Newman MG. Anxiety and depression as bidirectional risk factors for one another: A meta-analysis of longitudinal studies. Psychol Bull. 2017;143(11):1155.
Fainman D. Examining the relationship between anxiety disorders and depression: main topic. CME: your SA J CPD. 2004;22(10):568–71.
AN A, DA A, AT EASHMBHA. A, An Arabic translation, reliability, and validation of patient health questionnaire in a Saudi sample. Ann Gen Psychiatry. 2017.
Dawood E, Habib F. Comparison of depression and anxiety between housewife and employed pregnant women. Int J Nurs. 2018;5(2):23–31.
Lojewski J, Flothow A, Harth V, Mache S. Employed and expecting in Germany: A qualitative investigation into pregnancy-related occupational stress and coping behavior. Work. 2018;59(2):183–99.
Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–7.
Fatima M, Parvez R. Comparison study of depression between career and housewives women. Int J Mod Social Sci. 2016;5(2):133–9.
Gurudatt N. Postpartum depression in working and non-working women. International Proceedings of Economics Development and Research. 2014;78(69).
Fall A, Goulet L, Vézina M. Comparative study of major depressive symptoms among pregnant women by employment status. Springerplus. 2013;2:1–11.
Lancaster CA, Gold KJ, Flynn HA, Yoo H, Marcus SM, Davis MM. Risk factors for depressive symptoms during pregnancy: a systematic review. Am J Obstet Gynecol. 2010;202(1):5–14.
Zahid A, Siddiqui M. Life satisfaction and Depression among Working and non-Working Women of Quetta City. Journal of Education And Humanities Research (JEHR), University of Balochistan, Quetta. 2023;16(2):114–9.
Holton S, Fisher J, Rowe H. Motherhood: is it good for women’s mental health? J Reprod Infant Psychol. 2010;28(3):223–39.
Yang H, Zheng X, Zhou R, Shen Z, Huang X. Fertility behavior and depression among women: evidence from China. Front Psychol. 2020;11:565508.
Wdowiak A, Makara-Studzińska M, Raczkiewicz D, Cyranka K. Reproductive problems and intensity of anxiety and depression in women treated for infertility. Problemy Prokreacyjne a Nasilenie Lęku i Depresji U Kobiet Leczonych Z Powodu Niepłodności. Psychiatr Pol. 2022;56(1).
Alamri HS, Algarni A, Shehata SF, Al Bshabshe A, Alshehri NN, ALAsiri AM, et al. Prevalence of depression, anxiety, and stress among the general population in Saudi Arabia during Covid-19 pandemic. Int J Environ Res Public Health. 2020;17(24):9183.
Friesen K, Peterson WE, Squires J, Fortier C. Validation of the Edinburgh postnatal depression scale for use with young childbearing women. J Nurs Meas. 2017;25(1):E1–16.
Bawahab JA, Alahmadi JR, Ibrahim AM. Prevalence and determinants of antenatal depression among women attending primary health care centers in Western Saudi Arabia. Saudi Med J. 2017;38(12):1237.
Alqahtani JS, Oyelade T, Aldhahir AM, Alghamdi SM, Almehmadi M, Alqahtani AS, et al. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis. PLoS ONE. 2020;15(5):e0233147.
Steptoe A, Shankar A, Demakakos P, Wardle J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc Natl Acad Sci. 2013;110(15):5797–801.
Al-Hejji Z, Al-Khudhair M, Al-Musaileem M, Al-Eithan M. Prevalence and associated risk factors of antenatal depression among women attending antenatal clinics in primary health care centers in the ministry of health in Al-Ahsa City, Saudi Arabia. J Family Med Prim Care. 2019;8(12):3900–7.
Piirtola M, Kaprio J, Baker TB, Piasecki TM, Piper ME, Korhonen T. The associations of smoking dependence motives with depression among daily smokers. Addiction. 2021;116(8):2162–74.
Mykletun A, Overland S, Aarø LE, Liabø HM, Stewart R. Smoking in relation to anxiety and depression: evidence from a large population survey: the HUNT study. Eur Psychiatry. 2008;23(2):77–84.
Villanueva-Blasco VJ, Villanueva-Silvestre JMM, Vázquez-Martínez V. A. Relationship Between Depression and Risky Alcohol Consumption in Women: the Mediating Role of Coping Styles and Age. Int J Ment Health Addict [Internet]. 2024;22(3):1376–93. Available from: https://doiorg.publicaciones.saludcastillayleon.es/10.1007/s11469-022-00931-w
Lee HJ, Han DH, Lee YS, Kee BS, Kwon HJ, Park DB. Anxiety, impulsiveness, and drinking problems in employed women. Anxiety Mood. 2011;7(2):73–8.
Staehelin K, Bertea PC, Stutz EZ. Length of maternity leave and health of mother and child–a review. Int J Public Health. 2007;52:202–9.
Hyde JS, Klein MH, Essex MJ, Clark R. Maternity leave and women’s mental health. Psychol Women Q. 1995;19(2):257–85.
Dagher RK, McGovern PM, Dowd BE. Maternity leave duration and postpartum mental and physical health: implications for leave policies. J Health Polit Policy Law. 2014;39(2):369–416.
Avendano M, Berkman LF, Brugiavini A, Pasini G. The long-run effect of maternity leave benefits on mental health: evidence from European countries. Soc Sci Med. 2015;132:45–53.
McGovern P, Dowd B, Gjerdingen D, Moscovice I, Kochevar L, Lohman W. Time off work and the postpartum health of employed women. Med Care. 1997;35(5):507–21.
Acknowledgements
Not applicable.
Funding
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R218), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Author information
Authors and Affiliations
Contributions
DA, SA, and AA participated equally in Conceptualization, Methodology, Validation, Investigation, Writing– Original Draft Preparation, and Visualization. Formal Analysis, SA; Writing– Review & Editing, DA, SA, and AA; Supervision, DA; Project Administration, DA and SA; Funding Acquisition, DA.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted following the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of Princess Nourah bin Abdulrahman University (IRB log number: 21–0494) in accordance with the Declaration of Helsinki. Informed consent was obtained from all subjects involved in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
AlAteeq, D., AlNujaim, S.M. & AlGharbi, A.H. Prevalence of depression and anxiety among working women in Saudi Arabia: psychosocial and perinatal correlates. BMC Women's Health 25, 228 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12905-025-03776-2
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12905-025-03776-2